blog tambre
Polycystic ovary syndrome: symptoms, fertility and its new proposed name as PMOS

Table of contents
Polycystic ovary syndrome, known until now as PCOS, is one of the most common hormonal conditions in women of reproductive age. However, its name has caused confusion for years, because many patients understand it to mean that they have “cysts” on their ovaries, when in reality these are not pathological cysts.
What is usually seen on an ultrasound scan are small follicles that have not completed their maturation and have not released an egg. This ultrasound image is what historically led to the term “polycystic ovary”, but today we know that this condition is much broader.
For this reason, a recent publication proposes an international change in terminology: PCOS would become PMOS, standing for Polyendocrine Metabolic Ovarian Syndrome. In Spanish, this can be translated as síndrome ovárico metabólico poliendocrino, or SOMP.
This change does not mean that patients have a different disease. What changes is the way it is named. And naming it more accurately helps us understand it better: we are not talking only about ovaries, nor only about fertility, nor only about irregular periods. We are talking about a hormonal, metabolic and ovarian condition that can affect each woman differently.
In some patients, PCOS/PMOS appears as irregular menstrual cycles, acne, increased body hair or hair loss. In others, it is associated with insulin resistance, a higher risk of type 2 diabetes, high cholesterol, obesity or cardiovascular problems. And, from a reproductive point of view, it can make ovulation more difficult and make achieving pregnancy more complex.
Even so, it is important to convey a clear message: having PCOS or PMOS does not mean that a woman cannot become a mother. With an accurate diagnosis, appropriate follow-up and personalised treatment, many women with this condition do achieve pregnancy.
What is PCOS or polyendocrine metabolic ovarian syndrome?
PCOS, now proposed as polyendocrine metabolic ovarian syndrome (PMOS), is a condition that can alter ovarian function, hormonal balance and metabolism.
Traditionally, it has been described based on three main characteristics: irregular menstrual cycles, excess androgens — hormones that are also present in women, but at lower levels — and ovaries with a polycystic appearance on ultrasound.
However, this definition fell short for many patients. The new name aims to better reflect the clinical reality:
- Ovarian, because ovarian function remains important.
- Metabolic, because insulin resistance and increased cardiometabolic risk may be present.
- Polyendocrine, because several hormones are involved, not only those directly related to the ovary.
In other words, PMOS should not be understood only as a gynaecological problem. It can affect the menstrual cycle, the skin, metabolism, weight, ovulation, fertility and also emotional wellbeing.
As with other syndromes, not all women experience the same symptoms or with the same intensity. Some seek medical advice because of irregular periods, others because of acne or excess hair growth, others because they are having difficulty getting pregnant, and others discover the diagnosis during a routine gynaecological check-up.
For this reason, the approach must always be individualised.
Why is the name changing from PCOS to PMOS?
The change in name is being proposed because the term polycystic ovary syndrome can be inaccurate and confusing. The word “polycystic” suggests that the main problem is cysts on the ovaries, when in reality what is often observed are immature follicles, not cysts in the usual medical sense.
This difference matters. If a patient believes that everything comes down to “having cysts”, she may not receive a complete explanation of what is happening in her body. Attention may also focus only on the ovarian aspect, leaving hormonal, metabolic or emotional aspects of the syndrome in the background.
The new term, polyendocrine metabolic ovarian syndrome, aims to describe more accurately a condition that is complex, common and highly variable.
For some time, both names will probably coexist: PCOS, because it is the term most familiar to patients and professionals, and PMOS, because it better reflects current knowledge of this condition.
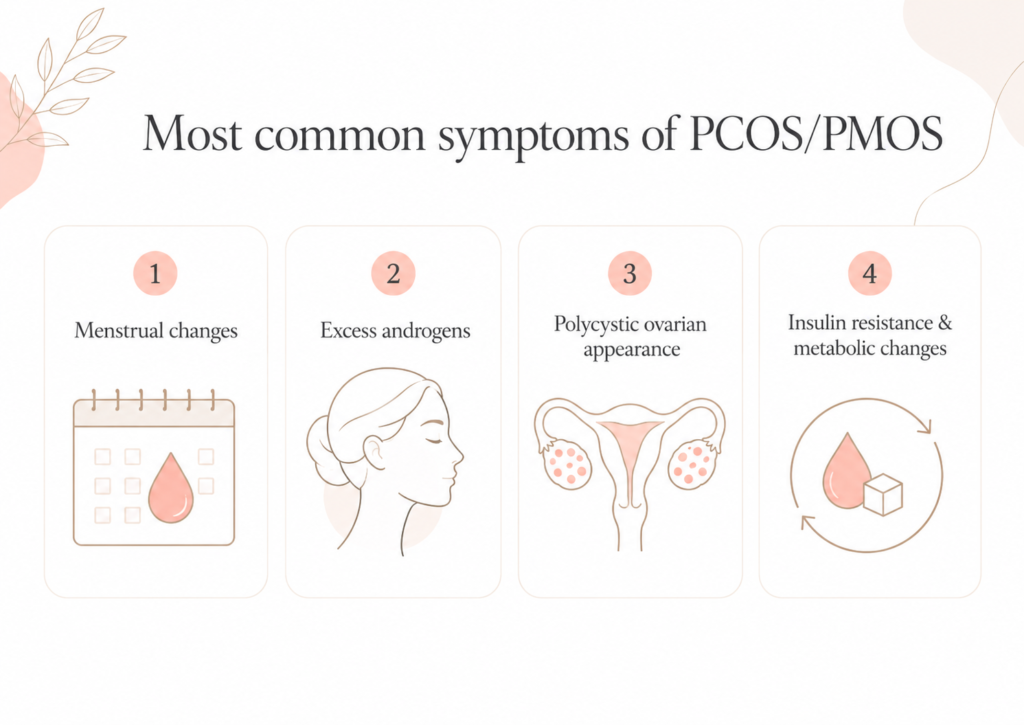
Most common symptoms of PCOS/PMOS
The symptoms of polycystic ovary syndrome or polyendocrine metabolic ovarian syndrome can vary greatly from one woman to another. In some cases, they appear during adolescence; in others, they are detected later, especially when the patient begins trying to conceive.
1. Menstrual changes
One of the most common signs is irregular menstrual cycles. Some women have very widely spaced periods, others may go for periods of time without menstruating and, in some cases, heavy or prolonged bleeding may occur.
These changes are usually related to irregular ovulation or the absence of ovulation, which is known as anovulation. If the ovary does not release an egg regularly, the chances of pregnancy decrease, because there are fewer real opportunities for fertilisation throughout the year.
In addition, when cycles are long or unpredictable, it becomes more difficult to identify the fertile days.
2. Excess androgens
Hyperandrogenism, meaning increased androgen levels, is another characteristic manifestation of PCOS/PMOS. It may be detected in a hormonal blood test or appear through visible symptoms.
Among the most common are hirsutism, persistent acne and hair loss with an androgenic pattern.
Hirsutism consists of hair appearing in areas where it is usually more common in men, such as the face, chest, abdomen or back. Acne may be persistent and may not respond well to conventional treatments. Hair loss, known as androgenic alopecia, may be perceived as a loss of density on the top of the head.
These symptoms do not only have a medical dimension. They can also affect the patient’s self-esteem, body image and emotional wellbeing. That is why it is important to address them sensitively and not minimise them.
3. Ovaries with a polycystic appearance
On ultrasound, some women have ovaries with multiple small follicles. Traditionally, this image has been described as “polycystic ovaries”, although in reality these are not true cysts.
These follicles have not completed their maturation and remain in the ovary without ovulating.
However, having ovaries with this ultrasound appearance does not necessarily mean having PCOS/PMOS. There may be women with polycystic ovaries on ultrasound who do not have hormonal changes, irregular periods or fertility problems.
Therefore, an ultrasound scan alone is not enough to diagnose the syndrome. It is necessary to assess the full picture: symptoms, medical history and hormonal results.
4. Insulin resistance and metabolic changes
Many patients with PCOS/PMOS have insulin resistance. This alteration can favour weight gain, make weight loss more difficult and increase the risk of type 2 diabetes.
In addition, insulin resistance can influence hormonal balance and favour increased androgen production, which may worsen symptoms and further alter ovulation.
This is one of the reasons why the new name includes the word metabolic. The syndrome does not only affect the ovary; it may also have implications for a woman’s general health in the short, medium and long term.
Why does PCOS/PMOS occur?
The exact cause of PCOS/PMOS is not fully known. It is currently considered a multifactorial condition, in which different elements may be involved.
One of these is genetic predisposition. It is common to find a family history of irregular cycles, hormonal problems or reproductive difficulties.
Hormonal imbalances also play a role, especially excess androgens and changes in the hormones that regulate ovulation.
Finally, insulin resistance plays an important role in many patients. When the body produces more insulin to compensate for this resistance, androgen production in the ovary may be stimulated, helping to maintain the cycle of hormonal and ovulatory alterations.
How can PCOS/PMOS affect fertility?
PCOS/PMOS is one of the most common causes of ovulatory infertility. This does not mean that all women with this diagnosis will have problems getting pregnant, but it can make the process more difficult.
The main reason is anovulation. If there is no ovulation, there is no egg available to be fertilised. And if ovulation occurs only in some months, the opportunities for pregnancy are reduced.
In addition, irregular cycles make it more difficult to calculate the fertile window. In women with very long cycles, it can be complicated to know when ovulation occurs or even whether it has occurred.
Metabolic changes are also involved. Insulin resistance can influence the hormonal environment and increase androgen levels, which may worsen ovarian function.
In some cases, endometrial receptivity may also be affected. The endometrium, which is the inner lining of the uterus where the embryo must implant, depends on appropriate hormonal coordination. When there is a significant hormonal alteration, this preparation may not be optimal, which could influence embryo implantation.
For all these reasons, when a woman with PCOS/PMOS wishes to become pregnant, it is important to study her case thoroughly and not limit the approach simply to “regulating the period”.

Treatment of PCOS/PMOS
Treatment depends on the patient’s symptoms, age, metabolic situation and whether or not she wishes to try for pregnancy at that time.
The objective may be to regulate cycles, improve symptoms related to excess androgens, reduce metabolic risks or promote ovulation.
Lifestyle changes
In many patients, especially when there is overweight, obesity or insulin resistance, lifestyle changes can play an important role.
A balanced diet, regular physical exercise and weight loss when indicated can improve insulin sensitivity, help regulate menstrual cycles and favour ovulation.
In some women, weight reduction may be enough to restore ovulatory cycles without the need to start medication. This is not about blaming the patient, but about understanding that metabolism and ovarian function are closely connected.
Pharmacological treatment
When lifestyle changes are not enough, or when symptoms require a specific approach, different medications may be used.
In women who are not trying to conceive, hormonal contraceptives can help regulate the menstrual cycle and reduce symptoms associated with excess androgens, such as acne or hirsutism.
In patients with insulin resistance, metformin may form part of the treatment. This is a drug used in metabolic alterations that can help improve the body’s response to insulin and, in some cases, support better ovarian function.
When the patient wishes to become pregnant, medications can be used to induce ovulation. These treatments may be oral or injectable and allow follicular development to be stimulated in order to increase the chances of ovulation and schedule sexual intercourse or assisted reproduction treatments.
In vitro fertilisation and PCOS/PMOS
When pregnancy is not achieved with simpler treatments, or when there are other associated fertility factors, it may be necessary to resort to in vitro fertilisation (IVF).
In patients with PCOS/PMOS, IVF can offer good results, but it requires particularly careful medical control. The reason is that many women with this condition have a high ovarian reserve and an intense response to hormonal stimulation.
High anti-Müllerian hormone
In PCOS/PMOS, anti-Müllerian hormone (AMH) levels are usually high. This hormone is produced by the small follicles in the ovary and is commonly used as a marker of ovarian reserve.
In a patient with PCOS/PMOS, a high AMH may indicate that there are many follicles available. This can facilitate the retrieval of oocytes during IVF treatment.
However, a high AMH does not necessarily mean greater spontaneous fertility. Although there may be many follicles, the main problem may still be the lack of regular ovulation or an altered hormonal environment.
For this reason, AMH must always be interpreted within the clinical context of each patient.
Risk of ovarian hyperstimulation
One of the most important aspects in patients with PCOS/PMOS is the risk of ovarian hyperstimulation.
During IVF or artificial insemination, medications are used to stimulate the ovaries. In women with many antral follicles, the response may be excessive if the dose is not properly adjusted.
Ovarian hyperstimulation can cause discomfort and, in severe cases, renal, hepatic or thrombotic complications. For this reason, in patients with PCOS/PMOS, cautious protocols, lower medication doses and close ultrasound and hormonal monitoring are usually used.
When a risk of hyperstimulation is considered to exist, a common strategy is to carry out the ovarian puncture, fertilise the oocytes obtained and vitrify the embryos. The transfer is performed later, once the ovary has returned to normal and the patient is in better condition.
This strategy helps reduce risks and protect patient safety.
Risk of multiple pregnancy
In ovulation induction or artificial insemination treatments, it is essential to monitor how many follicles are growing. If too many follicles mature, the risk of multiple pregnancy increases.
For this reason, in patients with PCOS/PMOS, very carefully adjusted medication doses are used and frequent monitoring is carried out. If an excessive response is observed, it may be necessary to cancel the cycle and recommend avoiding unprotected sexual intercourse.
In in vitro fertilisation, however, the risk of multiple pregnancy does not depend on PCOS/PMOS itself, but on the number of embryos transferred. For this reason, single embryo transfer is an important tool to reduce this risk.
PCOS, PMOS and pregnancy: a message for patients
The change in name from PCOS to PMOS should not cause alarm. If a patient already had a diagnosis of polycystic ovary syndrome, this does not mean that her diagnosis has changed or that she has a new disease. What changes is the way we understand and explain it.
The old name focused too much on the image of the ovary and on the idea of “cysts”. The new term, polyendocrine metabolic ovarian syndrome, helps remind us that this condition can involve hormones, metabolism, ovulation, fertility, skin, weight and general health.
PCOS/PMOS can make trying to conceive more difficult, but it should not be understood as a definitive diagnosis of infertility.
Many women with this condition become mothers, either spontaneously after improving ovulation, with ovulation induction treatments or through assisted reproduction techniques such as in vitro fertilisation.
The key is to make an accurate diagnosis, assess not only the ovaries but also metabolism, hormones, the endometrium and other possible fertility factors, and design a plan adapted to each patient.
At Tambre, PCOS/PMOS is approached from an integrated perspective: studying the origin of the alterations, personalising treatments and caring for both effectiveness and safety. Because in assisted reproduction, it is not only about starting a treatment, but about understanding each case properly in order to choose the most appropriate path.
Although PCOS/PMOS can create uncertainty, it is also a condition for which we now have many medical tools. With the right support, accurate information and specialist follow-up, it is possible to improve the reproductive prognosis and move towards pregnancy with greater confidence.
Do you have PCOS/PMOS and are you trying to conceive?
At Tambre, we study each case individually to understand how your hormones, metabolism, ovulation and other possible fertility factors may be involved. An accurate diagnosis helps us choose the most appropriate treatment and move forward with greater confidence.
Request a personalised assessment